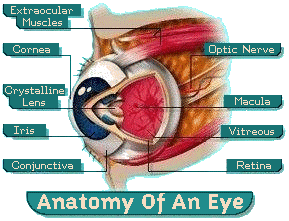
The Cornea and Cornea Conditions
The cornea is the eye’s outermost layer. It is the clear, dome-shaped surface that covers the front of the eye. Although the cornea is clear and seems to lack substance, it is actually a highly organized group of cells and proteins. Unlike most tissues in the body, the cornea contains no blood vessels to nourish or protect it against infection. Instead, the cornea receives its nourishment from the tears and aqueous humor that fills the chamber behind it. The cornea must remain transparent to refract light properly, and the presence of even the tiniest blood vessels can interfere with this process. To see well, all layers of the cornea must be free of any cloudy or opaque areas.
The corneal tissue is arranged in five basic layers, each having an important function. These five layers are:
Epithelium
The epithelium is the cornea’s outermost region, comprising about 10 percent of the tissue’s thickness. The epithelium functions primarily to: (1) Block the passage of foreign material, such as dust, water, and bacteria, into the eye and other layers of the cornea; and (2) Provide a smooth surface that absorbs oxygen and cell nutrients from tears, then distributes these nutrients to the rest of the cornea. The epithelium is filled with thousands of tiny nerve endings that make the cornea extremely sensitive to pain when rubbed or scratched. The part of the epithelium that serves as the foundation on which the epithelial cells anchor and organize themselves is called the basement membrane.
Bowman’s Layer
Lying directly below the basement membrane of the epithelium is a transparent sheet of tissue known as Bowman’s layer. It is composed of strong layered protein fibers called collagen. Once injured, Bowman’s layer can form a scar as it heals. If these scars are large and centrally located, some vision loss can occur.
Stroma
Beneath Bowman’s layer is the stroma, which comprises about 90 percent of the cornea’s thickness. It consists primarily of water (78 percent) and collagen (16 percent), and does not contain any blood vessels. Collagen gives the cornea its strength, elasticity, and form. The collagen’s unique shape, arrangement, and spacing are essential in producing the cornea’s light-conducting transparency.
Descemet’s Membrane
Under the stroma is Descemet’s membrane, a thin but strong sheet of tissue that serves as a protective barrier against infection and injuries. Descemet’s membrane is composed of collagen fibers (different from those of the stroma) and is made by the endothelial cells that lie below it. Descemet’s membrane is regenerated readily after injury.
Endothelium
The endothelium is the extremely thin, innermost layer of the cornea. Endothelial cells are essential in keeping the cornea clear. Normally, fluid leaks slowly from inside the eye into the middle corneal layer (stroma). The endothelium’s primary task is to pump this excess fluid out of the stroma. Without this pumping action, the stroma would swell with water, become hazy, and ultimately opaque. In a healthy eye, a perfect balance is maintained between the fluid moving into the cornea and fluid being pumped out of the cornea. Once endothelium cells are destroyed by disease or trauma, they are lost forever. If too many endothelial cells are destroyed, corneal edema and blindness ensue, with corneal transplantation the only available therapy.
Common corneal diseases include Allergies, Dry Eye, Fuchs, Keratoconus and Shingles
Keratoconus
The cornea is the window of the eye. Light travels through the cornea past the lens to the retina and then the brain to form a visual image. The normal corneal surface is smooth and aspheric i.e. round in the center, flattening towards its outer edges. Light rays passing through it moves in an undistorted manner to the retina to project a clear image to the brain.
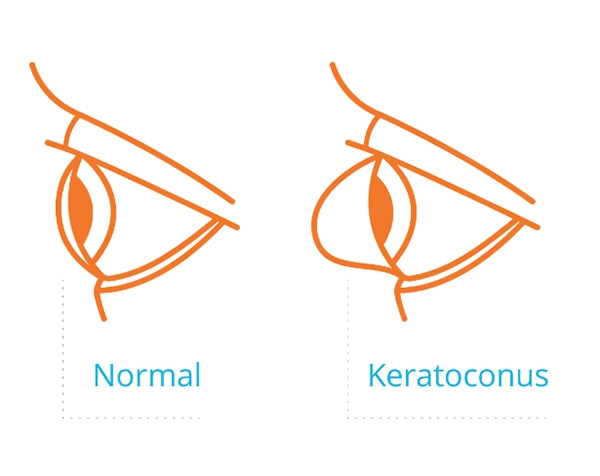
What Is Keratoconus?
Keratoconus, often referred to as “KC,” is a sight-threatening eye disease in which the typically round dome-shaped cornea progressively thins and weakens, causing the development of a cone-like bulge and blurry or distorted vision. This can result in significant visual loss and may lead to a corneal transplant if left untreated.
Symptoms
Keratoconus typically first appears in individuals who are in their late teens or early twenties, but can affect older adults too. Each eye may be affected differently. In the early stages of keratoconus, people might experience:
- Mildly blurred vision
- Frequent prescription changes
- Excessive eye rubbing
- Difficulty seeing at night
- Frequent headaches
- Vision that cannot be fully corrected with glasses or contact lenses
The cornea is responsible for focusing most of the light that comes into the eye. Therefore, abnormalities of the cornea, such as keratoconus, can have a major impact on how an individual sees the world, making simple tasks such as driving a car or reading a book very difficult.1
Keratoconus:
- Can result in significant vision loss
- May lead to corneal transplant in severe cases
- Affects both males and females
- Affects all ethnicities with some studies showing higher incidence rates among Asian, black, and Hispanic populations2
- 10% of people with KC have affected relatives3
- An estimated 5-30% of people with Down syndrome are also affected by keratoconus4,5
You can find more information at www.livingwithkeratoconus.com.
What Is iLink Corneal Cross-Linking?

iLink corneal cross-linking is the only FDA-approved cross-linking treatment for progressive keratoconus. It is a minimally invasive outpatient procedure that combines the use of ultraviolet light and specially formulated eye drops to stiffen and strengthen the cornea that has been weakened by disease or refractive surgery. Cross-linking is considered the standard of care around the world for progressive keratoconus and corneal ectasia following refractive surgery.6
Detailed content for the first and only FDA-approved cross-linking procedure can be found at https://www.glaukos-ilink.com/
Is iLink Covered by Insurance?
The medical necessity of iLink has become widely recognized. As a result, commercial insurance coverage for the procedure is now over 95% in the United States.
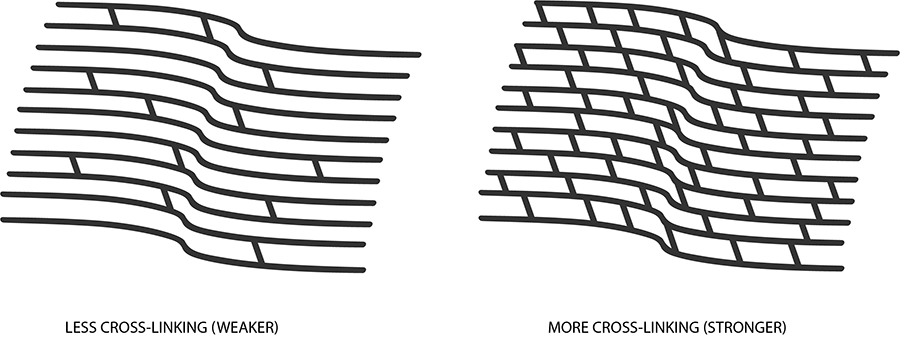
Corneal Cross-Linking7
- Creates new corneal collagen cross-links
- Results in a shortening and thickening of the collagen fibrils
- Leads to the stiffening and strengthening of the cornea
Riboflavin
During the iLink cross-linking procedure, specially formulated pharmaceutical-strength riboflavin eye drops called Photrexa® (riboflavin 5’-phosphate ophthalmic solution) and Photrexa® Viscous (riboflavin 5’-phosphate in 20% dextran ophthalmic solution) help enable the cross-linking reaction.
Ultraviolet Light (UV)
iLink corneal cross-linking applies ultraviolet light from a machine called the KXL System once the cornea has been soaked in the Photrexa® and Photrexa® Viscous eye drops. This process works to stiffen the cornea by increasing the number of molecular bonds, or cross-links, in the collagen.
Combining Riboflavin and UV Light
Using Photrexa® and Photrexa® Viscous riboflavin eye drops, combined with ultraviolet light from the KXL system, the iLink procedure stiffens and strengthens the cornea to slow or halt the progression of keratoconus and preserve vision.
Is Cross-Linking Right for Me?
Patients who have been diagnosed with progressive keratoconus or corneal ectasia following refractive surgery should ask their doctor about iLink corneal cross-linking.
Our practice is proud to offer patients the first and only FDA-approved therapeutic solution for the treatment of progressive keratoconus. Now, patients who once had little to no therapeutic option to treat keratoconus have the opportunity to slow or halt the progression of this sight-threatening disease.
For more information about the iLink procedure for the treatment of progressive keratoconus and corneal ectasia following refractive surgery, visit www.glaukos-iLink.com.
Photrexa® Products and KXL System Photos
Please feel free to use any of the high-resolution photographs we have included in the link. Please note these images provided are for your practice website or social media accounts, solely for the purposes of educating patients on KC and/or the iLink procedure.
IMPORTANT SAFETY INFORMATION
Ulcerative keratitis, a potentially serious eye infection, can occur. Your doctor should monitor defects in the outermost corneal layer of the eye for resolution.
The most common ocular side effect is haze. Other ocular side effects include inflammation, fine white lines, dry eye, disruption of surface cells, eye pain, light sensitivity, reduced sharpness of vision, and blurred vision. The risk information provided here is not comprehensive. To learn more, talk to your healthcare provider.
Go to glaukos-iLink.com to obtain the FDA-approved product labeling.
You are encouraged to report all side effects to the FDA. Visit www.fda.gov/safety/medwatch-fda-safety-information-and-adverse-event-reporting-program, or call 1-800-FDA-1088.
APPROVED USES
Photrexa® Viscous (riboflavin 5’-phosphate in 20% dextran ophthalmic solution) and Photrexa® (riboflavin 5’-phosphate ophthalmic solution) are used with the KXL® System in corneal cross-linking to treat eyes in which the cornea, the clear dome shaped surface that covers the front of the eye, has been weakened from the progression of the disease keratoconus or following refractive surgery, a method for correcting or improving your vision.
Tell your healthcare provider if you are pregnant or plan to become pregnant.
References:
1. National Keratoconus Foundation.
2. https://www.nature.com/eye/journal/v14/n4/pdf/eye2000154a.pdf
3. http://www.kcglobal.org/p/keratoconus.html
4. Alio JL, Vega-Estrada A, Sanz P, et al. Corneal morphologic characteristics in patients with Down syndrome. JAMA Ophthalmology. 2018;136(9):971-978.
5. Kristianslund, O, Drolsum, L. Prevalence of keratoconus in persons with Down syndrome: a review. BMJ Open Ophthalmol. 2021;6(1):e000754.
6. Gomes JAP, Tan D, Rapuano CJ, et al. Global consensus on keratoconus and ectatic diseases. Cornea. 2015;34(4):359-369.
7. Beshwati IM, O’Donnell C, Radhakrishnan H. Biomechanical properties of corneal tissue after ultraviolet-A-riboflavin crosslinking. J Cataract Refract Surg. 2013;39(3):451-462.
Fuchs’ dystrophy is a slowly progressing disease that usually affects both eyes and is slightly more common in women than in men. Although doctors can often see early signs of Fuchs’ dystrophy in people in their 30s and 40s, the disease rarely affects vision until people reach their 50s and 60s.
Fuchs’ dystrophy occurs when endothelial cells gradually deteriorate without any apparent reason. As more endothelial cells are lost over the years, the endothelium becomes less efficient at pumping water out of the stroma. This causes the cornea to swell and distort vision.
Eventually, the epithelium also takes on water, resulting in pain and severe visual impairment. Epithelial swelling damages vision by changing the cornea’s normal curvature, and causing a sight-impairing haze to appear in the tissue. Epithelial swelling will also produce tiny blisters on the corneal surface. When these blisters burst, they are extremely painful.
Shingles
This infection is produced by the varicella-zoster virus, the same virus that causes chickenpox.
Be aware that corneal problems may arise months after the shingles are gone. For this reason, it is important that people who have had facial shingles schedule follow-up eye examinations.